



1.5 Case Recording |
Contents
1. Introduction
| 1.1 | This policy, procedure and best practice guidance for case recording provides the framework and guidance for all aspects of recording for best outcomes for individual children and young people. All sections are mandatory and apply to all staff who contribute to case records for individual children and young people. There are three sections with appendices for ease of reference. |
2. Policy
2.1 Overview |
|
| 2.1.1 | Isle of Man Department of Health and Social Care, Children and Families Division believes that robust, timely and ethical record keeping is central to the provision of quality services which are safe and transparent and which promote the best outcomes. Managing, recording and interpreting case information is a skilled professional activity that both promotes and reflects quality practice. It is integral to the overall service to each child or young person and their family and is not an optional extra. |
| 2.1.2 | Children and Families is therefore committed to ensuring that case recording is consistently high quality, informed by evidence and a key part of effective and accountable professional practice. |
2.2 Definition of a Case Record in Children and Families |
|
| 2.2.1 | The social care case record is the “story” of the professional work and decision-making with or on behalf of a child. It is an integral part of the process of achieving best outcomes for each child or young person receiving a social care service. The case record refers to all the documentation appertaining to the child. |
| 2.2.2 | The record is part of the life story of each child and therefore is a key document which explains clearly for the future, what has happened and the reasons for decisions and actions. |
| 2.2.3 | The record enables clarity, reflection, communication, critical thinking, partnership working and sound decisions informed by evidence. |
| 2.2.4 | The record is cumulative over time, is stored and can be retrieved and shared at any stage. It is electronic and includes those documents which have been written, drawn, photographs, diagrams and audio or DVD recordings. These will have been uploaded to the electronic record. |
2.3 Ownership of Case Records |
|
| 2.3.1 | Case records of children receiving social care services are the property of the Isle of Man Department of Health and Social Care, which has the duty to maintain and share them according to the law and Departmental policy. |
| 2.3.2 | The individual whom the record concerns has the legal right to see their file in line with the Access to Records Procedure. |
2.4 Purpose of Recording |
|
| 2.4.1 | Recording is intended to be a dynamic tool to support and promote good practice, decision-making and outcomes and to demonstrate activity and accountability through the following:
|
2.5 Principles and Values |
|
| 2.5.1 | The record provides a clear, comprehensive and value based account of all aspects of the work done with children and decision-making. |
| 2.5.2 | The record is about and for the child and therefore the child’s “voice” must be loud and clear in the record. It is important that the record does not become too focused on the adult’s issues but at the same time a “whole family” approach is needed on the principle that support for those in a parenting role is an essential part of helping a child. |
2.6 Legal Requirements |
|
| 2.6.1 | Case records must comply with and reflect the following:
It is unlawful for a person, on racial grounds to treat another person less favourably than he treats or would treat other persons. These requirements clearly affect case recording.
These requirements clearly affect case recording. |
2.7 Confidentiality of Case Records |
|
| 2.7.1 | Case records contain personal data and sensitive information and therefore must be kept strictly confidential. This means that electronic records must be password protected. Contents must not be available to or disclosed to anyone without consent of the subject of the record other than to: the individual the record concerns as appropriate, employees and partner professionals with appropriate permissions to access them solely in order to provide a service or for management and quality assurance purposes or as directed by a Court. Any sharing or electronic record with others via email should be password protected. |
2.8 Information Sharing |
|
| 2.8.1 | Sharing of any individual and case information must be in accordance with the Isle of Man Safeguarding Board (IoM SB) website - Information Sharing. |
3. Procedures
3.1 Overview |
| 3.1.1 | This section describes the procedures and the systems which provide the framework for recording. They are designed to promote and support safe, effective and reflective practice and decision-making informed by sound evidence. The framework is to be used pro-actively to record, retrieve and use information to inform practice and decision-making in the child’s interests and as a means to achieve the best outcomes possible. Recording must not be seen as an optional addition to practice or an end in itself or merely as “form filling”. |
3.2 Recording Requirements in Children and Family Service |
|
| 3.2.1 | For interventions and decisions to be safe and effective it is essential that information recorded and retrieved about the child and their family is as complete and accurate as possible. |
| 3.2.2 | See Appendix 1: Responsibilities to Complete Templates in Protocol. |
3.3 Electronic Recording |
|
| 3.3.1 | All children and young people who receive a service will have an electronic file. Information completed on paper such as information from service providers, letters and specialist reports will be uploaded to the Protocol electronic record. This will primarily hold all ICS documentation, demographic information and running Case Notes. In addition to these, documents prepared electronically within Department of Health and Social Care must be uploaded to sit with the child/young person’s electronic Protocol record e.g. Court Reports, Secure Panel paperwork, minutes of meeting held outside the ICS processes, letters etc. There is no requirement to print off and hold in the paper file such documents, or ICS documents unless the practitioner wishes to for taking to meetings or other purposes. Emails which support a decision or action may be either, printed and added to the child’s file, or uploaded onto the relevant record. |
| 3.3.2 | All paper documentation received regarding a child/young person must be uploaded to the Protocol record. If key documents are received such as a specialist assessment; a Case Note must be created on Protocol to note the existence of the uploaded document. |
| 3.3.3 | If due to capacity further file/s are required, the allocated Social Worker is responsible for ensuring that the Protocol record is amended to reflect the relevant end date of the current file (via the ‘Update Record’ link) and open a record for the new file (via the ‘New Record’ link) with the correct start date and location. |
| 3.3.4 | The first and main point of reference for those who wish to find information (e.g. demographic information, allocation details) regarding a child/young person who is in receipt of services from Children and Families will be the electronic Protocol record. |
| 3.3.5 | Identification (ID) Number. Each child or young person referred for a social care service has a unique and permanent Identification Number given by Protocol at the point of referral. |
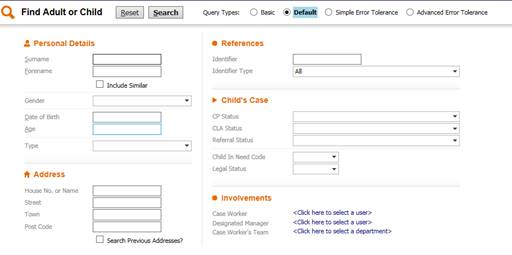
| 3.3.6 | It is essential that all demographics for a child and the child’s family and carers is correct and kept current. This is particularly important in respect of addresses as many confidential and personal documents will be sent to a person’s address. When creating a new record or updating a new address the post code search should be utilised firstly. Using this method is the least time consuming and decreases the risk of an incorrect address being added to a record. The most efficient and secure way of searching for an address is to only enter the postcode, then search results. |
| 3.3.7 | When performing a search by surname, it could have been entered into the system with a different spelling. To make searching more accurate, enter the first few characters only followed by ‘wildcards’ - * or % - into each of the name fields. The same applies to forenames, care should be taken to consider the other ways the name could appear e.g. Bill/William, James/Jim. Using the wildcard with the forename will also capture anyone in the system with a middle name recorded. Do not input data into each field, less is best. Make use of the DOB field, not only when searching for a person but also to confirm that you have found the correct person. It is good practice to check the address, if the person has moved since the address was last recorded this allows you to spot any discrepancies. |
3.4 Protocol and the Integrated Children's System (ICS) |
|
| 3.4.1 | The Integrated Children’s System is a framework to support practitioners and managers in the key tasks. It is made up of four elements which are updated as required:
|
| 3.4.2 | Protocol is the database which contains essential information and ongoing records about a child and their family. |
| 3.4.3 | Within Protocol the following screens and functions are particularly important for the Social Worker to maintain and use in working with the family:
|
| 3.4.4 | When performing a search by surname, it could have been entered into the system with a different spelling. To make searching more accurate, enter the first few characters only followed by ‘wildcards’ - * or % - into each of the name fields. The same applies to forenames, care should be taken to consider the other ways the name could appear e.g. Bill/William, James/Jim. Using the wildcard with the forename will also capture anyone in the system with a middle name recorded. Do not input data into each field, less is best. Make use of the DOB field, not only when searching for a person but also to confirm that you have found the correct person. It is good practice to check the address, if the person has moved since the address was last recorded this allows you to spot any discrepancies. |
 |
|
3.5 Recording Out of Hours |
|
| 3.5.1 | Where the Out of Hours Duty Social Worker responds to a currently open case the details of the contact and actions taken, including timings, must be recorded on Protocol using Case Notes added to the child or young person’s records. An alert will then advise the allocated social worker/their manager that the record has been added. |
| 3.5.2 | Where the Out of Hours Duty Social Worker responds to a new situation they must add the child/young person and any immediate family members to Protocol, record a Contact and Referral and add any Case Notes of activity undertaken. If a NARRATES is required this outcome must be selected from the Referral and the starting a NARRATES task sent to the Initial Response Team’s Tray. |
| 3.5.3 | Where a child/young person has been received into care out of hours a paper copy (available in the Duty Bag) of the relevant sections of the Placement Information Record must be completed to ensure the minimum information and consent requirements are met. These details can then be transferred onto Protocol and the rest of the pro forma completed at a more convenient time. |
3.6 Roles and Responsibilities in Case Recording |
|
| 3.6.1 | All staff have a responsibility to contribute to records in accordance with this Policy, Procedure and Best Practice Guidelines. Particular responsibilities are:
|
3.7 Alterations to Records |
|
| 3.7.1 | A record is not normally altered once completed but where necessary must be changed to a) correct significant inaccurate facts which may affect decision-making or b) remove entries which are clearly inappropriate such as discriminatory language or defamatory remarks about colleagues. If this happens, the date, circumstances and who altered it must be transparent. The date and person responsible will automatically show on electronic records. If a significant decision is found to have been made on the basis of incorrect information or unproven/prejudiced information recorded as fact, the manager must review the case and take action accordingly, seeking legal advice if necessary. |
3.8 Recording about Adults on a Child's File |
|
| 3.8.1 | Recording specifically related to adults on a child's file is not allowed. |
3.9 Records of Service Users who are also Employees |
|
| 3.9.1 | Where members of staff or members of their family are service users or service providers it is essential that they can be sure that personal information is kept confidential within the organisation and only accessed and used by the staff who need to know for the purposes of providing the services. Selective access rights will be set up to such records on Protocol. A decision will be taken by the relevant manager whether the paper file needs to be held separately and details of its secure location recorded on Protocol. |
4. Best Practice Guidance
4.1 Best Practice Overview |
|
| 4.1.1 | This section provides a framework for the best practice and the skills required to achieve case records which are accessible and professional and suitable to be used in evidence as required. It applies as appropriate to all aspects of recording including essential family and household information and all interventions, decisions and processes from referral to closure. |
| 4.1.2 | A good case record is focused and written clearly, concisely and in neutral straightforward language to communicate the meaningful “story” and decision-making about a child or young person. It will provide evidence that enables the reader to quickly understand the child’s full circumstances, needs and possible risk factors and the basis for decisions made with the reasons and the outcomes intended. It will both demonstrate and promote the process of analytical and critical thinking, partnership working and inclusive practice and it will show the constructive use of organisational systems. |
| 4.1.3 | Case recording is, and has always been, an integral tool of professional accountable practice. It will contribute most effectively to the achievement of good outcomes where staff view and value it as a positive aid to practice and as giving a “voice” to a vulnerable child rather than as a distraction from the “real” job. It is essential to regard recording as part of the real job. |
| 4.1.4 | At first sight the techniques for recording may seem obvious - (“Surely all professionals know what to write and how to write it”). However a high level of skill and versatility is needed to reflect the complexity of the work with children and their families. The following sections outline the essential practice requirements for effective recording in Children and Families. |
| 4.1.5 | If you can always answer yes to all of these questions it is likely that you are already recording to a high quality and standard.
|
| 4.1.6 | In order order to achieve quality recording the records from referral to closure must follow these guidelines: |
4.2 Structure of Case Records |
|
|
|
4.3 Content which Reflects Best Practice |
|
|
|
4.4 Recording Style |
|
|
|
4.5 Recording in Specific Situations |
|
|
|
4.6 Use of Recording Tools |
|
|
|
5. Summary of Best Practice in Case Recording
5.1 Structure |
|
| 5.1.1 | A good case record is focused and written clearly, concisely and in neutral straightforward language to communicate the meaningful ‘story’, interventions and decision-making about a child or young person. It is to be valued as a positive aid to practice and giving a ‘voice’ to a vulnerable child. |
| 5.1.2 | Each record must demonstrate it is:
|
5.2 Content |
|
| 5.2.1 | Case recording must reflect best practice by demonstrating it is:
|
5.3 Style |
|
| 5.3.1 | A professional and accessible style is essential which is in:
|
| 5.3.2 | Use of recording tools. Genograms, Ecomaps and assessment tools in specific situations are encouraged to aid practice and recording. |
6. Responsibilities and Timescales for Completing Templates on the Integrated Children's System
| 6.1.1 | The Integrated Children’s System (ICS) is a framework and set of tools to support practitioners and managers to manage key tasks and the volume and complexity of information gained in the course of the work with vulnerable children, young people and their families. ICS is made up of three elements which are updated as required: a set of data requirements, templates and a web-based IT system (Protocol). The templates are used to record the process, decisions and outcomes of aspects of intervention with vulnerable children and young people. |
| 6.1.2 | The table below specifies who is responsible for completing each of the templates using information gathered from the child, their family and partner professional. The Team Manager, or other manager, with appropriate permission must authorise each template on ICS once it is completed. |
| 6.1.3 | The templates are arranged below to reflect the titles and listing used on the ICS System. |
7. Case Closure
7.1 Policy |
|
| 7.1.1 | Effective reviewing and closure of cases will ensure that:
|
| 7.1.2 | Therefore a case will be considered closed to Department of Social Care when the following steps have been completed:
|
| 7.1.3 | The following additional steps must have been taken prior to closure on cases where there have been allegations of deliberate harm to a child.
|
7.2 Procedure |
|
| 7.2.1 | In each supervision session, or at other appropriate times, Team Managers must consider the caseload of their workers to identify if any cases must be closed in line with the first bullet points at paragraph 7.1.1 above. |
| 7.2.2 | If cases for closure are identified the Case Closure process on Protocol must be invoked, ensuring that the tasks identified in paragraph 7.1.2 above are complete, particularly the notification of children/young people, families and other involved professionals. |
| 7.2.3 | Please see Protocol manual for how to close cases on Protocol. |
Appendix 1: Responsibilities to Complete Templates in Protocol
Click here to view Appendix 1: Responsibilities to Complete Templates in Protocol.
End